When the British people know the truth about the Midazolam murders and that those crimes were the result of government policy that is tantamount to targeted euthanasia, which is still a crime in this country, there will be nowhere for the Four Horsemen of COVID-1984 and their army of accomplices in white coats to hide from justice.
In relation to which I will elaborate by way of this PCP update, in an attempt to convey in words the indescribable, gut-wrenching horrors of the prima facie evidence we have now assimilated into PUB’s Private Criminal Prosecution against everybody in the murderous Midazolam supply chain, which we will lay in a Magistrates Court at the earliest opportunity.
For the purposes of which, please watch the short video below, whether you’ve already seen it or not, so that you can fully appreciate the deservedly precarious positions which each of the defendants now finds themselves in.
Especially when we can now prove beyond reasonable doubt that, in the nefarious game of COVID-Cluedo, it was Hancock et al, in the cares homes, hospitals and the victims’ families’ properties, with syringes and syringe drivers full of Midazolam, the infamous benzodiazapine, which is used to varying degrees of success in lethal injections of Death Row prisoners in the US.
We also have an incendiary peer reviewed study which records that medical professionals within the NHS were reporting trends of fatal adverse events prior to the start of COVID-1984, after three patients died following overdoses of Midazolam between just 5 and 12mg.
Given that since then elderly and sick people have been injected with up to 60mg a day, only a fool could fail to see the plainly murderous intent of the defendants.
Anatomy of Genocide
During the second weeks of the scamdemic, Hull & East Riding Prescribing Committee distributed guidance on treating COVID symptoms, which stated that:
“For patients with distressing breathlessness at rest and unable to take oral medications, please consider starting continuous subcutaneous infusion via a syringe driver of:
Morphine sulphate 10mg + Midazolam 10mg subcut / 24hrs
OR if severe renal impairment (eGFR<30 mL/min): Oxycodone 5mg + Midazolam 10mg subcut / 24hrs (doses may need to be increased if severe symptoms; please ring palliative care team for advice).
NOTE: patients can still have additional PRN medications as required”
Fatal Symptom Management
In summary, they recommended giving subcutaneous 10mg doses of Morphine and Midazolam to patients suffering from severe breathlessness, using syringe drivers if they were not able to take the deadly drugs orally.
This is why so many of those who died as a result were first induced into comas, in order to prevent the administration of medicine by mouth; and almost always after they were forced to sign a Do Not Resuscitate notice, as their last conscious act and almost always without having any contact with their loved ones before their premature death.
Furthermore, the following passages are taken from the Hull & East Riding Prescribing Committee’s recommendations for assessing people with suspected COVID symptoms, which were in reality caused by the graphine oxide in the masks, the tests and the vaxxes imposed upon them prior to their diagnosis.
“Symptom assessment and rationale for selected management should be clearly documented. For patients approaching end of life, non-pharmacological management and care for the person/their family along with clear and compassionate discussions are key. Remind carers of the non-drug measures that can help symptoms – some suggestions included below. Please refer to local guidance and documentation for care of the dying person.
Yorkshire and the Humber End of Life Care Group drew up the regional guidance for the NHS, which became the guidance for dealing with ANYBODY they said had COVID symptoms, complete with the following disclaimer for insurance purposes:
These guidelines are the property of the Yorkshire and Humber Palliative and End of Life Care Group. It is intended that they be used by qualified medical and other healthcare professionals as an information resource, within the clinical context of each individual patient’s needs. The group takes no responsibility for any consequences of any actions taken as a result of using these guidelines. Readers are strongly advised to ensure that they are acting in line with current accepted practice and legislation, as these may change. These include, but are not limited to, The National Institute for Health and Care Excellence (NICE), the NICE guidance on the prescription of opioids, the British National Formulary (BNF) and the Palliative Care Formulary (PCF). No legal liability is accepted for any errors in these guidelines, or for the misuse or misapplication of the advice presented here. In difficult situations, please seek advice from your local specialist palliative care service.
The National Institute of Health and Care Excellence (NICE) have produced a central rapid guideline: Managing COVID‑19 for the management of individuals with COVID‑19 in all care settings (including end-of-life care).”
Midazolam Safety Warning
Neither Hull & East Riding Prescribing Committee nor NICE have any sustainable excuse for not knowing that Yorkshire and Humber HIEC and Yorkshire Quality and Safety Research Group published a report in January 2013, which drew urgent attention to the following Midazolam overdose warning, when it was being used as a component in anesthetic:
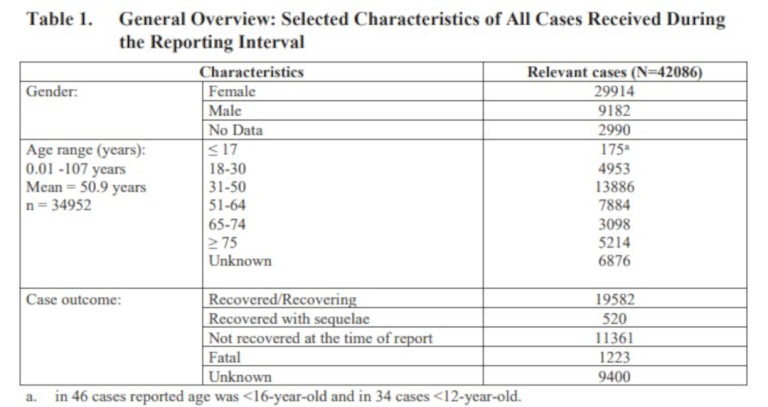
“In 2008 the National Patient Safety Agency (NPSA) issued a rapid response patient safety alert to reduce the risk of overdose with midazolam injection with adults (NPSA, 2008). This followed the receipt of 498 reported midazolam safety incidents between November 2004 and November 2008, whereby 3 patients died and a further 48 were moderately harmed.
Since the release of the alert, a further 417 incidents have been reported relating to wrong dose/strength errors, many (203) of which were related to administration of the medicine from a clinical area, and some (14) of which were related to monitoring/follow up (NPSA, 2012). The NPSA guidelines indicate that for adults, the intravenous injection of midazolam should be given slowly at a rate of approximately 1 mg in 30 seconds.
In adults below the age of 60 the initial dose is 2 to 2.5mg given five to 10 minutes before the beginning of the procedure. Further doses of 1mg may be given as necessary. In adults over 60 years of age, debilitated or chronically ill patients, the initial dose must be reduced to 0.5-1.0mg and given five to 10 minutes before the beginning of the procedure. Further doses of 0.5 to 1mg may be given as necessary (Roche Pharmaceuticals, 2008).”
Nevertheless, Hull & East Riding Prescribing Committee and its equivalent in every borough nationwide followed government approved NICE guidelines, which stipulated that the initial dose should be 2.5-30mg of Midazolam for symptoms of severe breathlessness, agitation or delusion, in any suspected COVID case, whether they be adult or child.
Moreover, those 3 deaths in 498 Midazolam safety incidents reported within the NHS extrapolates into a mortality rate of 0.6% [600 deaths for every 100,000 injections].
NICE Palliative & End-of-Life Care Guidelines
As alluded to above, the National Institute of Health and Care Excellence dictated that these guidelines be adopted by every health authority nationwide, to treat what they very broadly term agitation, restlessness and insomnia, in people of any age suspected of having or being likely to catch the government lurgy, all of which were experienced by the majority of Britain during the lockdowns.
“Agitation/terminal restlessness: Consider reversible causes (for example hypercalcaemia, constipation, urinary retention) and non-drug management If panic, anxiety and restlessness predominate – use benzodiazepine [of which Midazolam is one].
For altered sensorium with delirium, hallucinations, disorientation and disturbed sleep/wake cycle – use antipsychotic..
Oral: Haloperidol 500microgram to 1.5mg 4 hourly PRN Lorazepam 500microgram sublingual PRN (maximum 2mg in 24 hours).
Buccal: Midazolam can be used under specialist advice.
Subcutaneous: Haloperidol 1.5mg stat or 1.5 to 5mg/24 hours in a driver.
Levomepromazine 12.5mg stat or 12.5-50mg/24 hours in syringe driver.
Midazolam 2.5-5mg stat or 10mg -30mg/24 hours in syringe driver.
Higher doses of both drugs can be used under specialist advice.
Benzodiazepines may cause a paradoxical increase in agitation.
Midazolam 2.5-5mg stat or 10mg -30mg/24 hours in syringe driver” for agitation, restlessness or insomnia. Higher doses under specialist advice.”
These UK Government approved guidelines were drawn up and issued by NICE in full knowledge of the National Patient Safety Agency warning about the lethal dangers of over prescribing Midazolam in amounts above 0.5 – 2.5mg across all cohorts.
Given Hancock’s sworn confession to the House of Commons COVID inquiry, in which he confirms that he had procured, ordered and engaged enough Midazolam, Morphine, syringe drivers and the NHS staff to administer the lethal doses, in order to give the murder victims what Dr Luke Evans MP called “a Good Death” – a term which is synonymous with euthanasia – it’s no wonder that he was thrown to the lions in the aftermath of these undeniable facts being publicly exposed, in addition to the high court judgments against him for handing lucrative PPE contracts to his friends and family.
However, I hereby preemptively prescribe that the lives of the former secretary of state, the other three of the Four Horsemen and their endless stream of conspiring accomplices are about to become a whole lot more agitated, restless and sleepless, on the basis that we now have prima facie evidence which proves every single element of the most serious crimes that have ever been perpetrated.
Preemptive Prescribing at the End of Life
Indubitably, NICE has emphatically shown that they are about as far from nice as one could possibly be [yet another Sabbatean inversion], by laying down what can only accurately be described an instruction manual for placing people of any age on the end-of-life pathway, before they are showing any signs of shuffling off this mortal coil.
Moreover, according to the Cygnus Report, this is the direct result a UK Government policy driven initiative to save as much money as possible on keeping people alive, when they are preemptively considered unworthy of that which they mistakenly believed they had a legal right to receive and arbitrarily placed on the end-of-life pathway to lethal injection.
“PRE-EMPTIVE PRESCRIBING AT THE END OF LIFE
These are a guide for prescribing for patients not currently requiring opioids or antiemetics. For other patients, please seek advice. More information can be found in guidance associated with My Care Plan.
Morphine sulfate 10mg/mL injection 2.5 to 5mg sc hourly PRN
For pain or dyspnoea Supply 10 (ten) x 1mL ampoules
Midazolam 10mg/2mL injection 2.5 to 5mg sc hourly PRN
For agitation, distress or dyspnoea Supply 10 (ten) x 2mL ampoules
Hyoscine butylbromide 20mg/mL injection 20mg sc hourly PRN
For respiratory secretions or colic Supply 10 x 1mL ampoules Seek advice over 120mg/24 hours
Haloperidol 5mg/mL injection 500microgram to1.5mg sc 2 to 4 hourly PRN max 5mg/24 hours For nausea or agitation/delirium
Supply 5 x 1mL vials Seek advice over 5mg/24 hours”
Pre-emptive prescribing of Midazolam and Morphine to people not currently requiring them means prescribing in advance of either empirical diagnosis or the onset of symptoms, using the same drugs Dr Luke Evans MP stated [before the House of Commons COVID-19 inquiry in April 2020] were required for ‘a good death’, thereby guaranteeing the premature exit of many thousands of people.
Since we can adduce similar policy documents for every borough nationwide, the evidence of a thirteen year conspiracy to create an efficient administrative infrastructure to euthanize targeted demographics is now simply overwhelming.
Harrying of The North II
By way of a shocking example of that documentary evidence, the extract below is taken from the 2016 Palliative and End of Life Care Guidelines for Northern England, where there has been prolific Midazolam prescribing during COVID-1984, following five years of quietly implementing this genocidal policy of anticipating the onset of illness to justify the prescription of lethal pharmaceuticals.
“ANTICIPATORY MANAGEMENT
• Massive haemorrhage is often preceded by smaller bleeds. Oral/topical treatment may help (see below). When planning ahead, agree an Emergency Health Care Plan.
• Review risk: benefit balance of anticoagulants. Correct any coagulation disorder if possible.
• Consider referral for radiotherapy or embolisation if patient has an erosive tumour.
• Review resuscitation status and treatment options with patient and family. Document carefully.
• Dark towels should be available nearby to reduce the visual impact of blood if haemorrhage occurs.
• Prescribe anticipatory midazolam (10mg IV/IM/SC/buccal/sublingual) as a crisis one-off dose.
If resuscitation is inappropriate
• Try to remain calm. This will help a dying patient to achieve a peaceful death.
• The priority is to stay with the patient, giving as much reassurance/explanation as possible to patient and family.
• Use dark towels to absorb blood loss.
• Consider the use of crisis midazolam (10mg by appropriate route) to relieve distress in a patient that may be imminently dying.
RESTLESSNESS, AGITATION AND/OR DELIRIUM AT THE END OF LIFE
Consider and treat common causes of restlessness: eg urinary retention, faecal impaction and pain.
Support a calm environment, familiar voices and faces, gentle and usual routine.
Patients on regular or long term benzodiazepines should continue to receive a benzodiazepine. Give midazolam by SC infusion to prevent rebound agitation/withdrawal.
The doses given here are a guide. In complex situations seek specialist advice.
If patient is distressed or agitated, use midazolam.
Where there is delirium or to avoid excess sedation, use haloperidol.
Levomepromazine is an alternative for delirium, though more sedating.
Renal failure: Midazolam is a good first choice, as toxin accumulation increases seizure risk.
Anticipatory (Just in case) prescribing
Planning ahead is important even if a patient is not currently symptomatic: it is a risk in the dying phase.
Prescribe either midazolam 2.5mg SC 1-hrly as required (up to QDS), or Haloperidol 1.5mg SC 1-hrly as required (up to BD).
Doses should be titrated or regular treatment prescribed as below if symptoms develop.”
COVID-1984 Minority Report
All of which proves that it was and remains government policy to prescribe Midazolam [and Morphine] to people, with or without any symptoms of COVID-19, on the anticipatory presumption of a man or women in a white coat that they will in future contract and die from a cause of death which doesn’t exist and might never arise.
In other words, this is akin to witnessing a real life version of Minority Report, only instead of predicting crime and locking people up before they commit it, they are predicting death and murdering people who would otherwise live for days, weeks, months and years.
“Review within 24 hrs
If breakthrough doses needed, increase midazolam syringe driver dose by the equivalent of the extra doses given.
If midazolam dose > 30mg/24hrs – consider adding haloperidol 1.5 – 5mg/24 hrs SC or levomepromazine 25mg/24 hrs SC.
Continue breakthrough doses of midazolam 5mg SC 1-hrly as required.
Common dose range midazolam 10-60mg/24hrs (above this dose, seek advice).
Unresolved or severe symptoms
A few patients become extremely agitated when they are dying. This can be a very difficult situation and may require very high doses of medicines. Specialist advice should be sought. It is vital that patients are not left in distress.”
From which we can reasonably conclude that, in the event a patient becomes extremely agitated when they are preemptively placed on the end-of-life pathway, after testing false positive [or negative] for COVID-19, they are silenced with enough Midazolam to kill them.
That’s straight out of One Flew Over The Cuckoo’s Nest. However, rather than being the responsibility of a few errant health professionals, it is the direct result of a dictatorial government policy of eliminating the most resistant to their murderous ends, as well as the most vulnerable to such lethal preemptive prescriptions.
WHO Needs UK Needs Rounds
The WHO approved UK Needs Rounds policies were tested in Australia and when nobody realised in time to stop them proceeding unencumbered, its architects deemed it a success and it was imported here, as per the cartel’s plan.
Nevertheless,what the agenda amounts to is clearly mass murder by government policy, dressed up as a programme of social justice, care and compassion, so it’s about as heinous as one can get.
“Poor end of life care exposed by the pandemic
Covid-19 has had devastating effects on care homes across the UK. Disproportionate numbers of excess deaths have been recorded amongst care home residents and there are increasing reports of people dying alone. Discriminatory responses have included transferring older adults from hospitals to care homes, pressure to use do not attempt resuscitation (DNAR) / CPR orders, rationing according to age, and a lack of testing and PPE. This has significant justice and human rights implications, including the right to life, to health, and to non-discrimination.
Whilst issues of death and dying have undoubtedly been amplified by Covid-19, the need to improve care for people in their final weeks and days has been a priority for some time. Prior to the pandemic, up to 56% of care home residents died within the first year of admission and it is estimated that by 2040, care homes will be the most common place of death in the UK.
Yet, care home residents often experience poor end of life care as a result of avoidable hospitalisations, unmanaged symptoms, and inadequate communication, interdisciplinary working and advance care planning (ACP). This can be extremely distressing for residents and their relatives and must be urgently addressed.”
Damning 2020 Midazolam Study
However, despite the government policy of treating “unmanaged symptoms”[in hospitals, care homes and residential properties] with overdoses of Midazolam since April 2020, this damning study, published three months earlier, warned that the drug takes much longer to be cleared from the bodies of the elderly and the seriously ill to whom it has been routinely prescribed.
“One report in adult palliative sedation found mean midazolam doses of 29 mg/day (median: 30 mg, range: 15–60 mg/day).81 A recent study in an Israeli hospice found average doses of midazolam up to 79 mg/day.82 Mercadante and coworkers found mean doses were 23–58 mg/day.83 Midazolam is useful for palliative sedation in the home setting for pediatric patients.84 Initial doses were in the range of 0.02–0.08 mg/kg/h.84 Mean dose was 0.02–1.0 mg/kg/h.84 In treating terminal restlessness and agitation, Bottomley and Hanks15 used continuous infusion of subcutaneous midazolam in 23 advanced cancer patients in hospice. The investigators achieved symptom control in 22 of 23 patients using initial doses of 0.4–0.8 mg/h. The mean maximum dose was 2.9 mg/h. Dosing varied between patients highlighting the need to individualize dosing. Midazolam along with droperidol or olanzapine remains a treatment option for agitated patients in the emergency room.85
Adverse effects
Besides somnolence, most adverse effects are of low frequency.68 Clinical trials show that midazolam is safe to give with opioids for the treatment of dyspnea in advanced illness.69,70 Hiccups occur with an incidence of approximately 3.6%.71 Benzodiazepines cause disinhibition reactions to occur in both adult and pediatric patients, and midazolam is no exception.72 However, benzodiazepines in combination with antipsychotics help control delirium.73 Vorsanger and Roberts reported two cases of athetoid movements after receiving midazolam as a premedication.74 Physostigmine reversed the movement. Midazolam can cause prolonged anterograde amnesia.75–77
Advanced illness
Terminally ill patients experience significant physiologic changes affecting drug disposition. Loss of body weight and cachexia can lead to a decrease in Vd (volume of distribution). Decreasing Vd leads to increases in drug concentration and effect for lipophilic drugs like midazolam.32 Low albumin levels, commonly seen in advanced illness, decrease the clearance of midazolam.33
Elderly
Midazolam clearance decreases in the elderly. Prolonged elimination of half-life occurs in the elderly.34 Liver blood flow decreases with age, and midazolam is a drug with a low hepatic extraction (0.3), so elimination prolongs in low hepatic blood flow states.32,35″
Those last two paragraphs are very important, as the study concludes that Midazolam remains in the bodies of the most vulnerable cohorts for much longer than the other cohorts, which means that it takes much less to kill them than it does a healthy adult or child.
Nevertheless, the overdoses prescribed are pretty much identical to those recommended by the UK Government as a matter of public health policy, despite Midazolam never having been licensed for manufacture and distribution by the MHRA. In fact, the drug remains a ‘controlled substance’ under UK law.
But all they had to do to achieve their genocidal targets was put the old and sick on the end of life pathway, get them to sign a DNR and give them the recommended doses on the hour, until they were dead.
Which amounts to joint enterprise conspiracy to commit criminal fraud and mass murder by government policy.
A Nefarious Alibi For Mass Murder
Having said that, in this case we don’t have to prove fraud to proceed before a jury in a Private Criminal Prosecution any more because we are laying murder charges.
Nonetheless, the evidence we are adducing amply demonstrates that the fraud of COVID-1984 was concocted to provide the perpetrators of these truly heinous crimes with a plausible deniability.
In other words, they needed to manufacture the fake public health emergency so they could falsely claim everybody murdered with doctor prescribed Midazolam in the hospitals, care homes and in their own beds died ‘from’ or ‘with’ COVID-19, rather than from the potentially fatal illnesses they already suffered from, or didn’t, as the case may be.
Which necessarily means they needed the Coronavirus Act 2020 to lock the condemned inside care homes and their own domiciles, as well as to suspend autopsies on all suspected COVID deaths, otherwise the resulting postmortems would have revealed the killer drug’s abundant presence in the blood of the murder victims.
A profoundly nefarious alibi for mass murder, if ever there was one.
Heartfelt Gratitude (A message from Michael O'Bernicia)
Despite the heavy subject matter of this post, I can’t put a full stop on it without paying tribute to everybody who has supported my work over the past eighteen months, in whichever ways you have been able to.
Not only have you assisted in dramatically expanding of the reach of my content, which is currently seen by millions of people every month across all platforms, you have also helped keep all my content ad and paywall free for everybody, with the generous tips you have thrown in the Tips Jar, for which you will all soon receive an invitation to claim an equally generous reward in a new credit-based cryptocurrency [which is on the brink of launch] to show my appreciation.
In addition to all of that, this blog now has more than 15,000 subscribers, with a collective average engagement rate of 82% and an average IQ of at least 125; whilst my various social media platforms currently have in excess of 100,000 followers between them and the continue to grow rapidly every month.
Considering that we are living in an real life Idiocracy, in which critical thinking is bordering on a criminal offence, I am both honoured and humbled by the fact that so many critical thinkers are engaging in the increasingly wide dissemination of the eclectic and heavily censored work of a notoriously blacklisted, subversive Geordie recalcitrant, such as myself.
From the bottom of my heart, thank you to each and every friend, follower and subscriber. Never underestimate how essential your support, in whatever form it comes, is integral to the success of our mutual struggle to end the tyrannies which continue to abound on these ancient shores.
In The Names of The Midazolammed
No matter how much effort it requires, one day, sooner than you might think, we will all wake up in a land where the unalienable rights of the individual are protected from the tyranny of collective government.
In such a land, governed under the Common Law of Do No Harm But Take No Shit, the administration of the COVID-1984 Genocide would be a lawful and practical impossibility, which is why the Trustees of Universal Community Trust and myself will do all within our capability to bring about that outcome peacefully.
Nevertheless, to do so we must first indict all the defendants we allege have committed joint enterprise mass murder by government policy of an estimated 136,000 people, from April 2020 to June 2021.
For the purposes of which, please share this post far and wide, telling everybody you know that justice must and will be done, in the names of the victims who were #Midazolammed by UK Government policy
Original article published on The Bernician here


 text 1
text 1
 text 2
text 2
 text 2
text 2
 text 2
text 2
 text 2
text 2
 text 2
text 2